


This is a guest article by Doctor of Physical Therapy, Erika Mundinger, who gave a tremendous talk at The Fitness Summit in 2015 on how to deal with back pain caused by SI joint dysfunction. Her talk was one of the most popular of the weekend, and I knew this information would be helpful to other lifters and coaches so I asked her to put together an article for me. While there can be myriad causes of back pain, among experienced lifters it very often comes down to a lack of complete function in the SI complex, which these alternatives do a remarkably effective job at resolving. Hit us with the science, Erika…
It’s not news that 70-80% of the population has or will at some point experience dysfunction related to back pain. But back pain can come in many forms which can make dealing with it a bit tricky. Somewhere between 15-30% of the people with back pain of these people will have either an accompanying sacroiliac joint (SI) dysfunction or an isolated SI dysfunction. This can range from a minor ache to a completely disabling. When it comes to lifting weights, having SI pain can be downright scary. I hear weekly in the clinic “I can’t work out until this goes away.” Unfortunately, what we need to help our clients understand is that not exercising will certainly not help in resolving back pain. It doesn’t “just go away and fix itself” as some may want to believe, or as they may have been misinformed from an outside source. Most often there is a faulty movement pattern that occurs through the pelvis that will keep the problem at a low level smolder that may be almost undetectable only to have to it come back again a week, a month, a year later. On the other hand, exercising incorrectly will often aggravate back pain, putting people in a bit of a catch-22.
So we have no movement aggravating symptoms, yet moving may aggravate symptoms.
So what do we do? Ignore it? Hope it goes away anyway? Push through it? No pain no gain?
Where’s the middle ground? There has to be a way for not just physical therapists, but also for trainers and coaches, to help clients exercise both around pain and to CORRECT the associated causes of the pain in the gym aside.
While the typical home exercise program that involves just piriformis stretching, foam rolling, and clamshells is effective, there are more effective paths a lifter can take. (Note: These are beneficial exercises for SIJ dysfunction. Stay tuned for part II with more on at-home self maintenance exercises.)
First, it helps to understand how the SI joint moves mechanically.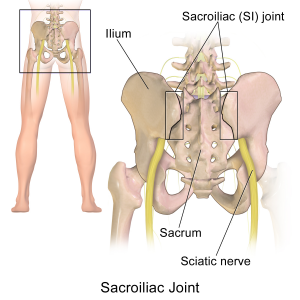
The SI joint and pelvis, like any other part of our body, moves on a three-dimensional axis. We can isolate each axis individually but for daily, functional movement, it moves simultaneously forward/back, side-to-side, and up/down. Think of walking for example. As one foot is forward the other foot is behind, the trunk rotates, the pelvis rotates, and one side will lift while the other side drops. Our muscles form “slings” around the pelvis working on longitudinal, horizontal, and oblique axes creating stability, also called force closure, from all directions.
Ok, so that sounds fancy and can get infinitely more complex if we were to break it down further. But what does this mean? In simple terms, to restore optimal mechanics in three dimensions it can help to train multi-planar movements.
How do I know it’s my SI, and not something else?
First, see your doctor. Typical SI symptoms will involve pain offset from the lower back, just above the hip and buttock. Pain will refer to the buttock, top of hamstring, and possibly around to the side of the hip. Symptoms will typically worsen with prolonged sitting, bending forward, bending forward and lifting heavy loads, and standing. Most people will feel better with walking and a bit of rotation. If this sounds like you, give these movements a try and see if you notice reduction in pain and better mobility. But again, these are “typical” symptoms and there is still variance from person to person. If symptoms are more localized to the spine itself, include pain shooting down the leg past the knee, or if you have numbness and tingling in to a specific area of your lower leg and foot, these may not be appropriate or productive exercises to try. And of course, if things aren’t improving, seek medical advice.
Without further ado, here are a few common exercises with correctional and rotational modifications to try with your current lifts.
Single Leg Deadlifts
Why it hurts:
This is a fantastic exercise to train the glutes, core, and hamstrings not to mention pelvic stability and balance. However, if we have a weak glute max and glute med, which is typically seen with SI dysfunction, the we get uneven closure of the SI joint from an unbalanced force locking system. We get excessive longitudinal pull through the SI without enough diagonal/oblique stability. The result is even more compression and shearing on an already painful joint.
The Fix: Single Leg Rotational Deadlifts
This exercise utilizes more glute med and piriformis than the single leg deadlift to help provide more uniform force closure. To perform this exercise, start with a kettlebell or dumbbell at the side of the foot, bend down rotating slightly to pick up the bell, and then stand up to a neutral position.

Please note, if you lack hip or spine mobility to comfortably twist to pick up the bell, or if balance is poor, elevate the kettlebell or dumbbell by placing a yoga block or a small step under the bell at the side of your foot so you don’t have to bend as far. The exercise will still be beneficial and will prevent any straining.
This exercise can also be done on two feet if balance is poor.
Lunge
Why it hurts: As with the single leg deadlift above, this is a single plane movement that relies on glute max, glute med, and hamstrings. While EMG studies have shown that there is more glute med and max activation with the single leg squat compared to the lunge, looking at activation alone can be misleading. In a single leg squat there is higher activation of glute med than the lunge, but there is a much greater activation difference between working and non-working leg. The result is a force differential that is significantly greater across a system that is already lacking the function to stabilize opposing forces. In other words, the single leg squat is too stressful and looking at activation of one muscle in isolation can be misleading as to how it contributes to the system. The net result is that the lunge is a better exercise, but we need to make it activate more glute med than in a normal lunge pattern – that only exacerbates the singular plane problem.
The Fix: Curtsy lunge
Similar to single leg rotational deadlift above, this exercise helps to activate more glute med and piriformis for SI mobility, not to mention the rotational movement of the exercise helps to retrain normal SI mechanics and rotation. Start with your foot on a Valslide, or furniture slider, or if on a hard floor have a towel under your sliding foot. As you slide your foot back, cross it behind you. As you stand back up think about engaging all the muscles around your hip to pull yourself back in to standing.

Kettlebell Swings
Swings are great for glutes, not to mention great for simultaneously getting a quick burst of cardio. But SI dysfunction sufferers tend to approach this move with a bit of trepidation and fear. This is one exercise I have heard clients at the gym commonly say “I wish I could do swings, but I always hurt too much after.”
The Fix: One-Handed Lateral Kettlebell Swings
This motion utilizes the spine’s natural rotation and fires a ton of muscles along the diagonal planes, engaging the glute max and med, obliques, and lats to name a few. Stand with your feet slightly wider than hip distance and staggered with one foot forward and one foot behind. Grab the kettlebell in the opposite hand of the forward leg (so if stance is staggered with right foot forward use your left hand to swing the bell). Perform a one-handed swing keeping the torso pointed forward but allow the hips to rotate slightly following the bell at a 45 degree angle from midline.


Fix Yo Biz
You may notice that when performing these movements that one side may feel easier on one side than another due to natural asymmetries and muscle imbalances. Also (disclaimer time) if you have limited rotation, be sure to start with low weight or no weight and focus on just doing the motion. Also never force more rotation than you can comfortably do. Starting with heavy loads or more rotation than available right off the bat with underlying dysfunction may exacerbate symptoms, but working through them with the focus on mobility can absolutely serve as a means to correct.
P.S. If these tips are helpful to you, you might find these tips helpful as well which are based on the same concept of how the SI functions and what causes and fixes this type of back pain.
Read it even on a Friday. Thanks for this! Eagerly awaiting part II.
Why are we attacking a flexibility issue with a combined strength/balance/range of motion set of exercises that most injured people will cheat their way through and not get the intended outcomes? If the exercise can’t be performed accurately, the potential positive result is lost.
If I’ve got a frozen SI, I won’t be able to do ANY of those exercises correctly, and their benefits will be blunted, if not entirely lost.
In my practice, unweighted (Range Of Motion) ROM exercise is more likely to effectively address these movement limitations.
Interested to hear your clinical observations of both effective and ineffective outcomes with various strategies. Why choose to add resistance beyond bodyweight when simply achieving correct ROM is such a challenge?
Perhaps we are simply dealing with different populations. I mostly work with mature adults >40 with serious ROM and pain issues. Maybe these techniques are more effective with <40 yr/old relatively fit folks? I'm curious to hear your clinical observations.
Thanks for the well written article!
Ben,
I’ll let Erika post her own response, but I’ll make three points.
1) It’s not a flexibility issue, it’s a function issue.
2) Added load is always individual, and there is no reason you can’t do these movements unloaded when appropriate.
3) That said, adding load is a good way to non-linearly influence tissue that has been formed under load and if not load, the repeated stresses of time. Very often, load is required to create enough of a demand to influence adaptation. With some people you can do all the unloaded movement you want, but it’s not going to overcome the specific adaptations to imposed demands of everything ELSE they did that got them there.
I hear you, but I don’t think that when there is inability to perform proper ROM under ANY condition loaded/unloaded that adding load is the way to smooth that out. So creating an artificial dichotomy of loaded/unloaded is incorrect.
Performing proper motion under ANY load condition is job 1. And unloaded gives us the chance to groove these motions most accurately. For my senior population, the load of bodyweight is more than enough to help groove the movement.
When I try to train a junior athlete, I start with proper motion and balance. With seniors, the initial training is no different… we just have to adjust to the pre-existing injuries and limitations. Proper ROM is job one. Strength through that ROM is job two.
I know I’m not alone in this opinion. And I know successful coaches who don’t hold with it. But they are competitive coaches, not people who work with the ordinary walking wounded. Those are my people, the folks just trying to perform the ordinary movements of life, who can’t even imagine performing fancy kettlebell exercises, let alone buying the things, or finding a gym that has them.
We can help the most by targeting the most. If it takes a foam roller or a kettle bell to accomplish it, most people will never experience it.
Ben,
Respectfully, now you’re just moving the goal posts. This article is very specifically intended for lifters, and was written for my audience that comprises people who lift and spend time in gyms as it is. You’re moving the goal posts by acting like it should be addressed to anyone and everyone. Context matters, and of course the intervention changes with the context.
I’m happy to continue the discussion with you privately, but I won’t discuss this any further here. You’re creating confusion and not adding any value to my readers.
Thank you. I didn’t mean to create any confusion between audiences. I regret any fuss as a result.
I simply answered in reaction to my experience with the general older adult population.
I developed an SI problem. I am an experienced cross trainer covered from many years of primary weight training. I am a man of a certain age. My SI problem developed as a result of several years of correcting my gait from walking feet angling out to feet straight in front of me. it took many years (6) for the change to travel up my muscular structure. First my first two metatarsals were extremely sore. Then the medial side of my knee. Ultimately after six years it culminated in what I am educated guessing was a realignment of my SI joint, the onset of which happened during a rigorous advanced kettlebell workout. At first it was just a slight twinge that was unremarkable. Over the next few weeks it became extremely painful, I could barely walk or sit. Like many, I decided I would wait for it to go away. Slowly pain diminished so that it was only episodic. After 3 months I was walking and running without pain but aware that there was activity in the joint. I did a few yoga classes, and I felt the joint settle in to its new reality, adjusted to a gait that is far better for the long term health of my hip and body. I got back in the saddle with kettlebell works with weights but concentrated on our form, slower deliberate engagements. It has been therapeutic. Yes, it does slightly increase the soreness of the joint after exercising, but the soreness feels good and right. And I am extremely happy to be exercising again. The takeaway here is that if one is experienced and/or well coached, David is 100% correct. Modified kettlebell exercise will hasten your recovery. Waiting it out just makes it worse. If one is inexperienced or not accustomed to training then yes unloaded exercises are prudent…. but without question less effective and will take a long recovery time.
Ben I agree with you, and it’s a great point about where we need to safely start. Elderly populations who lack mobility, adding weight would be detrimental rather than beneficial. In the clinical and rehab setting, unloaded is also absolutely a must at first. You simply can’t ascertain how much available motion there is unless you first know how a body moves unloaded. And absolutely despite the age of the athlete, young or old, if there is pain we will always start with body weight and ROM first. That’s also why I wrote the disclaimer at the end. If ROM isn’t available, adding load would create a problem. But someone who is a lifter who may have some SI dysfunction with some sticky spots in to rotation might find some benefit with playing around with loaded rotation. Again, not to be confused with just grab the heaviest load and rip it off the ground jerking as hard as you can! But if done mindfully with load progression they can often see a reduction in symptoms.
Part of the reason I chose these exercises was that you CAN train them unloaded, the deadlift and lunge anyway. I do variations of these lunges and deadlifts (more in the form of a rotational squat) unloaded in the clinical setting every day to train more mobility in the spine, SI, pelvis, and hip joints. They can be quite effective regardless of fitness level.
Glad you liked the article!
Hi Dr. Mundinger – I’ve had SI Joint Dysfunction for 30 years. I’ve played sports and worked at the gym all my life. But I could never gain muscle in my glutes simply because I could never load them with any exercise because the right SI joint would always pop out. Then, back to re-hab and bodyweight exercises until I felt strong enough to try again. Yup, every damned time I tried to load, it would pop out. I’ve given up so many times I’ve stopped counting. The set of exercises you have given here are amazing. I’ve got good ROM due to yoga and have been exceedingly careful of proper form. If you have any links to further weighted exercises for the SI Joint, I would be ever so grateful. I agree that a novice shouldn’t try these without guidance. With that said, there are many folks like myself who have never been able to push over the boundary of the dysfunction to build proper strength that exceeds body weight exercises. Please, keep up the good work!
I can’t wait to try these! Since attending the Biofeedback seminar last year, I’ve made all my lifts about what feels better instead of focusing on trying to be perfectly symmetrical. I love the Jefferson DL. Even with conventional DL and trap bar, I still stagger my feet whenever I feel like it, and it seems to work great for me. But of course, adding some new movements to the mix will only make it all more fun. Thanks!
I’ve carried lower back pain most of my life but it got better when I switched from loose forward to prop in rugby and I presume it was because of the forced compression on the spine that I found relief (I was in my 30s ) until I retired and then the pain started again. I then found exercises similar to compression to the spine and it gave relief until I started weightlifting a couple of years ago…back squats, bench press and deadlift and now progress has been slow lately because of exposed weaknesses in the lower back. I’m sure I can overcome these pains with the proper exercises you’ve described because the X-rays I had on the spine showed little reason for concern about excessive wear on cartilage but slight pinching of the nerve in one area and it’s never been a problem since learning to strengthen the core…..but this SI thing you mention could be my problem all along so I’m more than glad to start from here this week. It actually makes a lot more sense for my condition because I don’t want to give up lifting yet until I’m dead!! Thanks Dave. I know I haven’t told you everything about me yet but you will after I’ve trialled these exercises. Cheers, PapaRangi
I’m always looking for ways to help SI dysfunction, these exercises make a lot of sense, thank you! I always found that lying on a hard surface would cause my SI joint to lock up and eventually discovered I had a weak glute med on the opposite side. I never stopped exercising and it was painful to fix but once I adjusted to being a bit more balanced it’s been much more stable. Something I find useful when it slips out or locks up is doing a few single leg bridges on each side and doing some adduction and abduction with resistance, that usually pops it back in to place!
Hi,
Just tried these exercises and feel like they hit the spot!
Should I do them once a day? Or say 3 times a week? How many sets/reps would you recommend?
Do I need to do anything else? I’m generally pretty active otherwise – run and do a basic bodywork routine several times a week. I like the idea of identifying 3 or 4 compound exercises that – if I do them every day for however long it takes (weeks? months?) – will finally knock this SI thing on the head – have I found those exercises? Or should I also be doing clamshells, fire hydrants, quadraplexes, leg raises, stretches etc etc etc?! The list of exercises you could/should do is mind-boggling every site says different! I just want a simple, quick, realistic routine I can follow religiously to fix this pesky SI thing.
Many thanks in advance for any advice you can offer!
Rob
Rob, 2-3 times per week for around 3 sets of ten is probably a safe bet. Ideally you’ll want to test with biofeedback and wave the load and volume. One thing to note – there is NO routine that you can just religiously follow. Your body is constantly changing and you need variability, in fact a lack of variability is what causes this problem in the first place. You’ll have to change your mindset around it or you’ll always be chasing a solution and never finding resolution.
I have inflammation in both SI joints and both performis
One leg does not rotate in and one leg does not rotate out
Would these excercises be beneficial my issues.
Thanks
Pam, the only way to know is to test it out.
Hi David!
I am 27 year old female who was training Muay Thai when I must have slipped a disc. An MRI confirms a mild bulge. For 3 months doctors thought it was a hamstring strain because I only had symptoms in my legs, which I could not walk on without buckling. I lost a lot of strength during this time. For two months, I could use my left leg and I had sciatic nerve pain my right. After some rehab and recapturing of the disc, I ended up spraining my SI joint pretty severely doing very little weight (my mind didn’t realize how much atrophy my body went through. I know better now!). That was several months ago and progress has been slow but I am finally walking more and doing more strenuous rehab.
I couldn’t understand why progress was slow until you mentioned chain movements. My muscles are severely unbalanced from close to a year of me favoring my right side. I am excited to gently try these motions and see if they can help correct some of these dysfunctions.
I’ll be careful but I’ll let you know if I see any improvement. Anything that can get me at least up and running again would be an improvement!